Practicing at the Edge of ABO: Navigating Rare A Subgroups
- Jan 16
- 4 min read
Updated: Feb 5
There are moments in transfusion medicine when the most uncomfortable part of a case isn’t the serology — it’s the realization that the literature can’t quite tell you what to do.
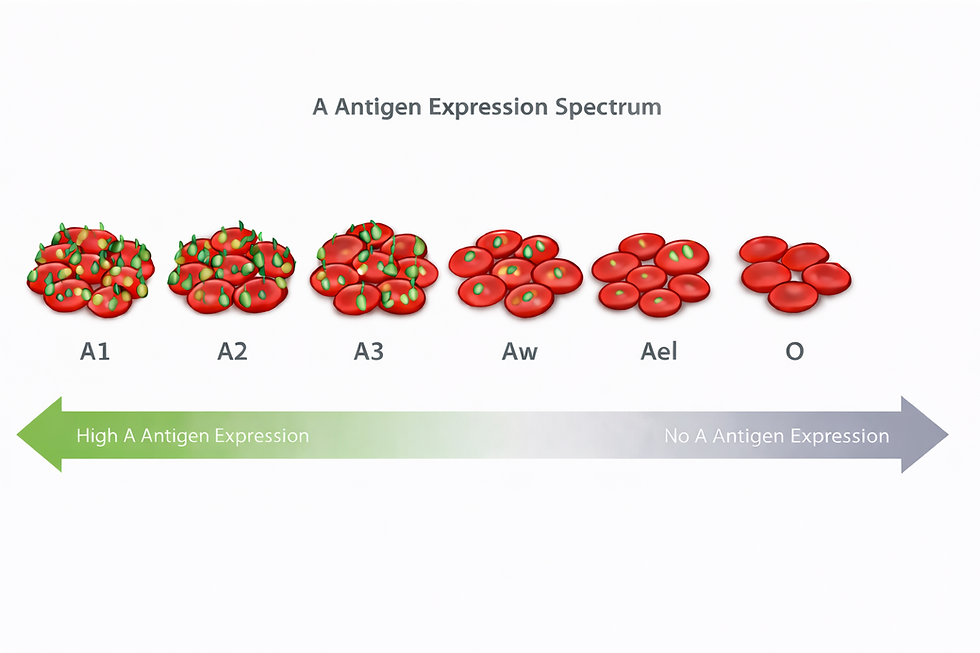
Recently, on service, I encountered a patient with a rare A subgroup and a cold-reacting anti-A1. Genotyping suggested either an Aw allele or an Ael allele. The immediate question was practical and deceptively simple: Is it safe to transfuse group A red cells, or should we restrict the patient to group O?
What followed was a familiar exercise for anyone who practices in the margins of evidence: reading case reports, revisiting mechanism, and trying to decide how much uncertainty is acceptable when the downside is fatal hemolysis.
Along the way, one thing became clear: not all weak A phenotypes are biologically — or clinically — interchangeable.
In particular, A3 is not the same as Aw, and neither is the same as Ael. Yet they are often discussed together, sometimes implicitly treated as a single category. That shortcut matters.
The problem with “weak A” as a single bucket
In everyday blood bank practice, weak A phenotypes are often grouped together for operational reasons: they may present as ABO discrepancies, require additional testing, or trigger conservative transfusion strategies.
But biologically, these phenotypes arise through very different mechanisms, and those differences shape how we should think about transfusion risk.
Here’s a simplified comparison.
A3 vs Aw vs Ael — why the distinction matters
Feature | A3 | Aw | Ael |
Typical serologic pattern | Mixed-field agglutination with anti-A | Weak or very weak anti-A; variable | No agglutination with anti-A |
Detectable without elution? | Yes | Often yes (weak) | No |
Detectable by adsorption–elution | Usually not needed | Sometimes | Required |
Underlying mechanism | Reduced or mosaic expression; often promoter/splicing effects | Hypomorphic A transferase with allele-in-trans–dependent expression | Near-null expression, often due to early truncation of A transferase |
Degree of A antigen exposure | Present on a subset of RBCs | Variable; can be extremely low | Trace only |
Evidence base for transfusion safety | Relatively robust (dominates “weak A” literature) | Sparse, case-based | Extremely limited |
Theoretical risk of allo-anti-A | Low | Uncertain | Plausible (no incidence data) |
Why A3 is different
A3 is classically defined by mixed-field agglutination with anti-A: some red cells express A antigen clearly, others do not. Importantly, A antigen is present and visible without elution.
From an immunologic standpoint, this matters. The immune system has likely been exposed to A antigen throughout life. Unsurprisingly, much of the reassuring transfusion experience for “weak A” phenotypes comes from cohorts dominated by A3 and similar variants.
When people say, “We transfuse A all the time in weak A and nothing happens,” they are often — implicitly — talking about A3.
Ael: a fundamentally different phenotype
Ael occupies the opposite end of the spectrum.
These phenotypes typically arise from premature termination codons early in the ABO A transferase gene. Routine serology shows no A antigen at all; detection requires adsorption–elution, and even then only trace amounts are found.
In practical terms, most circulating red cells are immunologically indistinguishable from group O.
Does this mean patients with Ael will form allo-anti-A? No one knows. The literature does not report an incidence. But mechanistically, the conditions that support immune tolerance to A antigen are clearly not the same as in A1, A2, or A3 phenotypes.
This is where the phrase “absence of evidence is not evidence of absence” stops being academic.
Aw: the uncomfortable middle
Aw phenotypes are what make this topic genuinely hard.
Unlike A3, Aw is not a mixed-field phenotype by default. And unlike Ael, it is not uniformly silent. Instead, expression depends heavily on the allele in trans.
One of the most striking demonstrations of this comes from maternal–child discordance cases, where the same Aw allele produced:
essentially no detectable A antigen when paired with an O allele, and
robust A expression when paired with a B allele.
In other words, Aw can look immunologically like Ael in one context and A2 or stronger in another.
When you encounter Aw in the blood bank, you are not just dealing with “weak A.” You are dealing with context-dependent A expression, and that uncertainty follows you into transfusion decisions.
What about hemolysis and antibodies?
Most anti-A1 antibodies are cold, IgM, and clinically insignificant. That’s true — until it isn’t.
Case reports exist of hemolytic transfusion reactions involving anti-A1 when thermal amplitude is broad or when additional risk factors are present. These cases are rare, but they loom large precisely because the denominator is so poorly defined.
What we don’t have are:
incidence data for allo-anti-A formation in Ael or Aw individuals,
outcome studies stratified by molecular subgroup, or
prospective evidence that transfusing group A is uniformly safe across all weak A genotypes.
So when clinicians default to group O in these cases, it’s not ignorance. It’s an acknowledgment of uncertainty.
Conservatism isn’t a failure of evidence — it’s stewardship
In my case, we chose to transfuse group O red cells while we waited for expert input. That decision wasn’t driven by panic or dogma. It was driven by a simple question:
If I’m wrong, what happens to the patient?
In transfusion medicine, the cost of being wrong is asymmetric. Hemolysis is rare — until it isn’t — and when it happens, it’s unforgettable.
Until we have better data, it is reasonable to treat A3, Aw, and Ael differently, even if our SOPs and textbooks sometimes collapse them into the same category.
Closing thought
Somewhere between genotype, phenotype, and patient safety is a space where we practice medicine without a net. That’s not a failure of science. That’s where judgment lives.
And sometimes, judgment looks like a unit of group O.
Please see this related post for an update on this case: https://www.bloodbytesbeyond.com/post/anti-a1-in-practice-not-in-theory



